
Practice Template
One of the great things about the modern PT student is their level of education. Current programs, with the occasional unfortunate exception, do a pretty good job giving a proper foundation of the scientific method and basic critical thinking. With our clinical interns, we also try and reinforce the purpose of their education is not to learn exactly how to treat like we do, but to learn how to think and evolve. My hope is that as the years go by, the exact details of what they use to treat their patients will change through critical thinking, just as mine do. But there is an inherent problem here. And this problem leads new graduates into the same reasoning traps as their predecessors…
When a student enters a clinical internship they are faced with a horrifying reality: A real live patient. All of the evidence and critical thinking in the world cannot prepare them for that interaction. How do you apply ALL of that information? They look to their clinical instructor for guidance which usually comes in the form of, “Here is what I do.” But clinicians commonly do something funny here. They apply a template that was either taught to them via continuing education (often a proprietary “system”, “approach”, or “method”) or a previous mentor, or was acquired via their own experience. It becomes “intuitive”. To explore the problem here, we are going to go to two quotes from Daniel Kahneman, a nobel laureate who is an expert on human decision-making.
“Whether professionals have a chance to develop intuitive expertise depends essentially on the quality and speed of feedback, as well as on sufficient opportunity to practice.”
“Short-term anticipation and long-term forecasting are different tasks, and the therapist has had adequate opportunity to learn one but not the other.”
– Daniel Kahneman
The experience of most clinicians is in short-term anticipation not long-term forecasting.
- The patient is evaluated
- The patient is treated
- The patient feels better
- The patient is discharged
- The next patient is evaluated
The assessment often looks for findings that anticipate a short-term, often immediate response to a particular treatment. As a matter of fact, many evaluative “systems” are specifically designed this way. They seek those immediate results and may even have some RCTs demonstrating those effects (be they specific or, most likely, non-specific effects). It is predictable and easily repeatable to the point that it becomes intuitive for the provider. This is very seductive to many students and new professionals and often the “best and the brightest” will adopt these approaches out of convenience. But many of these interventions are nothing more than clinical magic and placebos. Studies assessing the long-term forecasting of such treatments, something that most clinicians have ZERO experience with, are typically not very encouraging.
But students and new graduates need a template for how to approach their patients that is simple and timeless. Not some rigid “system” but one that will allow their practice to evolve with time while still applying the template. Not something that plays to short-term anticipation but rather addresses long-term forecasting.
So here is my template
This is what I teach my interns and other clinical instructors. It is a simple process of hierarchy that can be used no matter what the population is or your preferred practice philosophy. There are subjective and objective components to each section – I’m not going to get into those details. The goal is the important part. Again, a template, not a cookbook. What EXACTLY you look for and how you look for it will change over the years as our understanding evolves. But it should always fit this template.
Primary Exam
The first thing you are determining is the presence of the “sinister” things. These, of course, include your red flags. Those are easy and well defined. The other part is other potentially serious pathologies that you should be aware of. The question you are really asking is, “Should I refer this patient out for an additional consult?” I work in sports medicine so for me I am typically looking for signs and symptoms of large torn structures like ligaments, cartilage, etc. You may be looking for fractures, neurological compromise, psychological problems, etc.
In medicine, the process for determining this is classically a differential diagnostic procedure. You want to create a list, the differential, of all the possible things you could be seeing. Then you systematically rule them out. Why not rule in? Well because in science you FALSIFY, not confirm.
Now, we are not talking about “PT diagnoses” – we’ll establish that in the secondary exam. We are talking about things that may warrant, for example, a surgical consult. These tend to be specific diagnoses – “I believe you tore your ACL.” Now, just because you suspect something specific in your primary exam, it doesn’t mean you must make a referral. Current best-evidence will tell you that.
For example, you may highly suspect an acute meniscus tear. Since there are no signs of locking/rampant swelling, the current evidence suggests that conservative management is best at this time. No need to order a consult quite yet.
I find the primary exam to be the MOST IMPORTANT EXAMINATION SKILL-SET OF THE PHYSICAL THERAPIST. Know when you have significant pathology and when to make the appropriate referral. Keep in mind, you are not just looking for physical problems. For example, you may pick up on a potential major depressive disorder that requires a psychiatric referral.
To be honest, the majority of the patients that we see go on to the secondary exam without requiring an immediate referral, so let’s move on.
Secondary Exam
So you’ve gone through your primary exam and found that it is not necessary to refer this patient out. You now continue on to your secondary exam. Now, before we get all cute looking at movement, stability, or whatever you think is important today, let’s call a spade a spade. Our patients are dealing with one simple problem:
Something in the organism is not tolerating the demand being placed upon it.
Maybe this is a tendon. Maybe this is the nervous system. Maybe there are emotional factors. You see my point. The system is underperforming for some reason. So your secondary exam is to determine where the patient is at currently:
- Physically – What positions/movements do they tolerate? How much load can they handle?
- Mentally – How well are they educated regarding their situation?
- Emotionally – Are there more layers to their injury? Do they feel safe?
Your goal here is to establish your starting point. Your job is to get to their level on all three components so you have a known starting point for your intervention.
Goal Setting
You know where they are, now where do they need to be and by what date? These are their long-term goals. As the expert it is your job to advise them so that their expectations are realistic. Also, when you don’t know (we often don’t) be honest about it.
It is also your job just set very achievable short-term goals so that your patient can have quick success and stay motivated. It can also help you quickly identify when something is not going right and may need a new primary exam.
Intervention
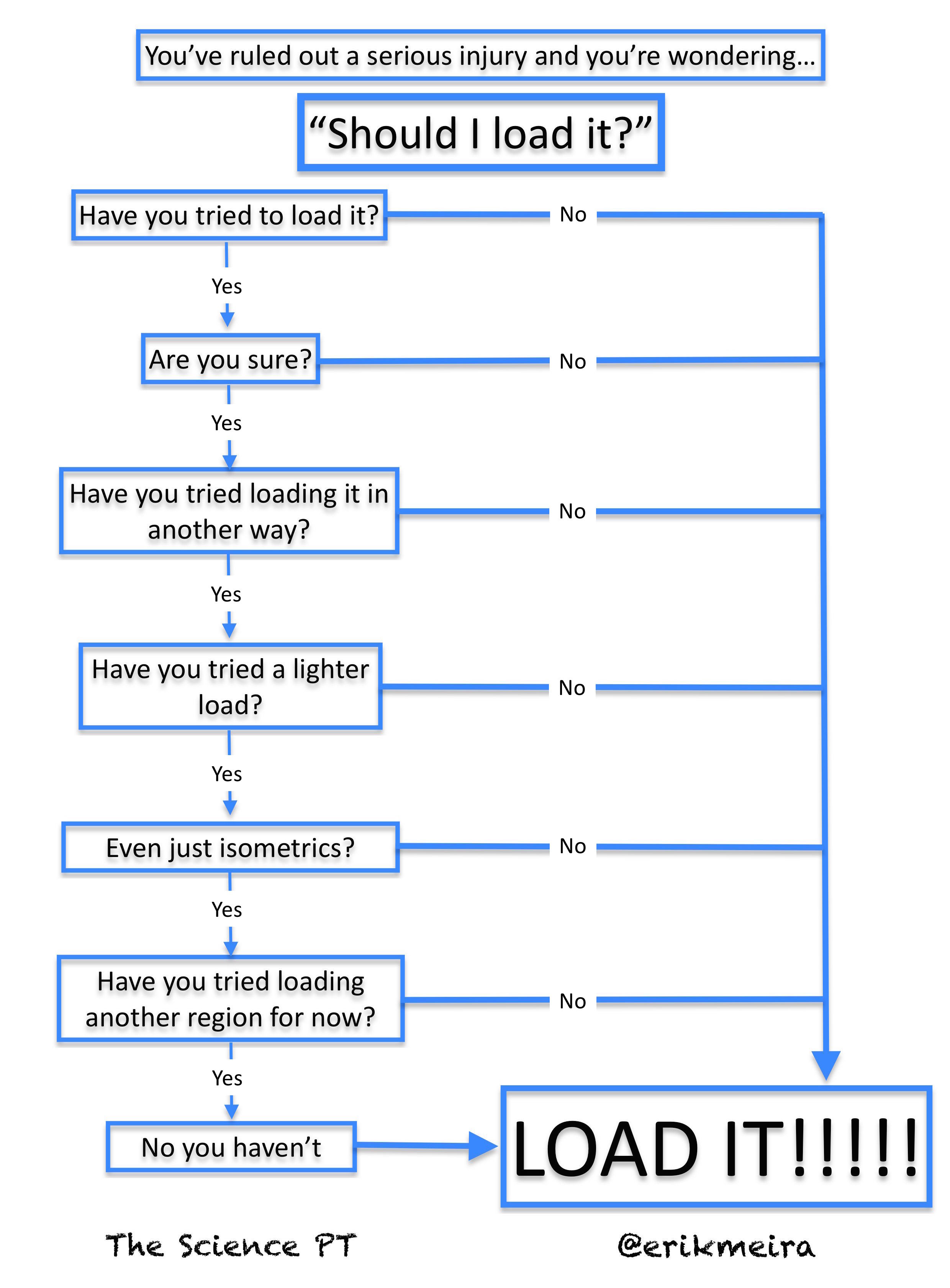
This seems to be weirdly complicated for a lot of clinicians which confuses me. Take where they are (established in the secondary exam) and progressively load them so they can adapt. Sometimes you do that by increasing reps per set. Sometimes by increasing the intensity or the speed. Usually it’s increasing all types of loads systematically while giving the organism time to adapt. This goes for the emotional components as well, typically through some kind of graded exposure with appropriate reassurance. Again, the details change as the research changes, but the template still fits.
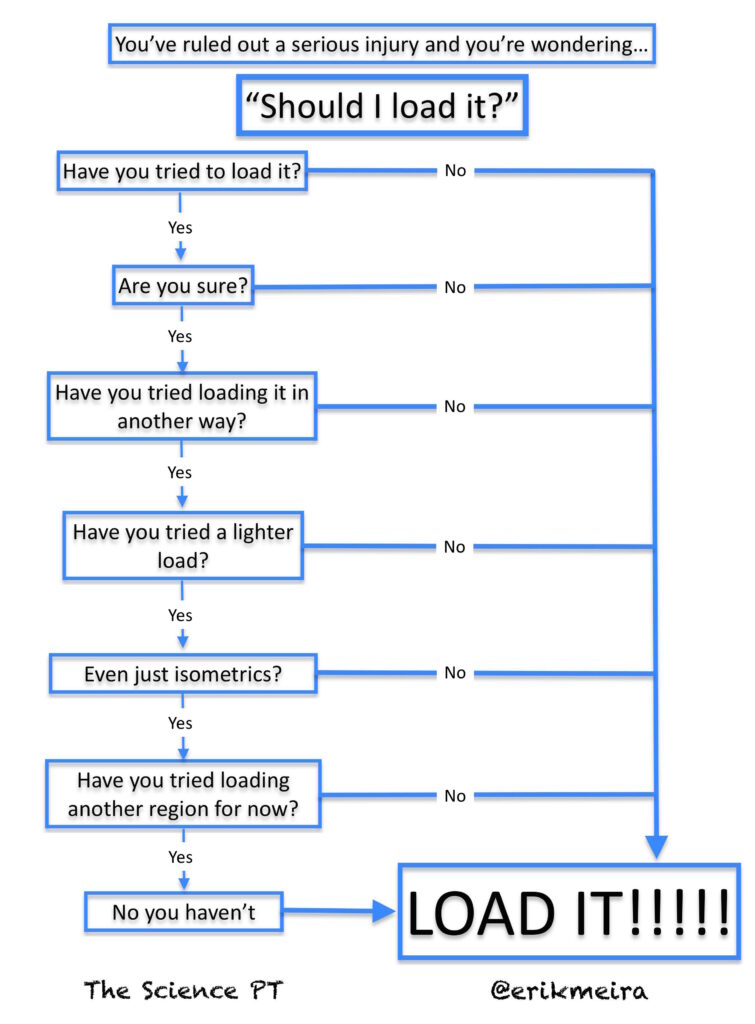
My handy flow chart. Click to embigginate.
You absolutely need to bring their load tolerance above the anticipated demands of their ultimate desired task. You may need to look at the task to make sure that they aren’t doing something REALLY goofy making the final demand unreasonable. I agree that this is a factor but I think that as a profession we overanalyze this concept. Get them adapting. Also, add some Placebo-fu.
And yes, there can be coordination factors, but that comes later – they need to tolerate more load first. And when you do want to change movement, that gets really complicated and specific.
Reassess
Every so often (usually once a month for long-term rehab) start from the top again for a reassessment. Has something more serious begun to present itself? Reestablish where they are physically, mentally, and emotionally. Assess their progress. Do you need to adjust those goals?
There you have it
That’s pretty much it. If you feel good about your critical thinking skills but don’t know how to apply them, just fit them into this template. It shows you the core questions that you need to ask yourself about the patient in front of you. Don’t make things more complicated than they need to be.
Also remember that there are a lot of ways to load people. Follow the research on how best to apply the details as our understanding progresses over time. One day it may point more to eccentrics. Maybe isometrics play a greater role or you should be incorporating rate of force development more. The point is that the details change, but the framework remains.
In summary…
- Our intuition is better at short-term anticipation than long-term forecasting – Don’t trust it!
- Rule out “the sinister” things that require immediate referral.
- Where is the patient physically, mentally, and emotionally? Start there.
- Set reasonable and achievable short-term goals.
- Apply progressive load and give time to adapt
- Don’t make things more complicated than they need to be.
The featured image on this post is “Should I Load It?” by Erik Meira and is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License
 .
.
{kind=link}