
Elite Level Placebos
Before we get started, my hope here is that even the hardest placebo skeptics and firmest placebo believers appreciate the points I make in this post and can agree with this way of thinking. I’m trying to be empathetic and understanding here. Don’t get me wrong – I’m not very happy about it and blood is coming out of my left ear. That said, I really hope both the believers and the skeptics have some things to think about after reading this…
CLARIFICATION FOR NON-USA READERS: In the United States we also have athletic trainers (AT) as another member of the sports medicine team. They are usually full-time employees of the school or team and typically are the ones managing day-to-day medical issues of the athletes. Often an AT is the one providing a lot of the treatments to which I am referring in this post.
The “training room” refers to their domain as opposed to the “weight room” where strength and conditioning (S&C) occurs. ATs are sometimes also licensed physical therapists but not always and that is not at all required. The AT will usually be the one to coordinate care between the physician, surgeon, and physical therapist then communicate with S&C, coaches, parents, administrators, etc.
Let me start by laying my cards on the table. I have been a licensed physical therapist since 1998. I have worked with athletes almost that whole time. About 15% of my current caseload can be considered “elite” the rest are high school, club, and recreational. I have spent my fair time in training rooms on college campuses at the Division I level. I have seen it all when it comes to crazy treatments.
Also, I have never performed cupping. I have also never performed dry needling (or whatever else you want to call acupuncture). I have never performed a spinal manipulation nor have I ever scraped someone with a tool. Never have I performed anything that would qualify as a massage or “soft-tissue mobilization” of any kind. I also have never done whatever thing you are currently thinking about that I haven’t even heard of yet, and probably never will.
When I say “never” I mean NEVER have I done any of these things to a patient, athlete or not. Even without ever doing these things I am still very popular with the athletes I work with. It is not uncommon to have an athlete say, “Please, can I talk to Erik about this.” I don’t bullshit. Everyone knows this. When I am done with an athlete, every one of them has a thorough understanding of what we know and don’t know about what they are currently going through. I am brutally honest. And I treat them all like adults who are not stupid.
I will admit to performing a patellar mobilization in 1999 and I still do the occasional long axis traction to a really irritated hip joint but that happens maybe once or twice a year and usually in an educational context (teaching a family member to do it). I have a “therapeutic” ultrasound machine somewhere in the clinic but I haven’t used it since 2003 and even then it was rare.
I do have an e-stim machine. I use it mostly for NMES to the quad during the 4 weeks after ACL reconstruction from the thinking of trying to minimize fat infiltration to that muscle, but I admit that this is conjecture and I don’t use it on every ACLR patient. I do, on occasion, wire it up for interferential current (*GASP!*) if a patient specifically requests it. I never offer it unsolicited, I clearly state that it is a placebo, and I do not bill for it. I have been known to offer an ice pack or ice massage (self-applied) even several weeks after an injury. Again, stated as a placebo and for no charge.
I also use isometrics fairly frequently for pain reduction which, I must admit, may be due more to “neurophysiological effects” (fancy way of saying placebo) than anything specific. Whatever your opinion on that (I’ve had my arguments), there is not a lot of research here on how isometrics relate to pain. I personally don’t have a full position yet.
Some of you may be thinking I’m a hypocrite – “How can you not do the things I love while still doing the things I hate?!” I’ll address this in a moment. The rest of you may be thinking that I’m a sell out – “How dare you perform ANYTHING that may be all placebo?!” Again, let’s leave the strawmen for the end. As I said before, I hope you both have some things to think about after reading this.
And of course some of you are coming from the “I do whatever the athlete wants!” perspective. No you don’t. There IS a line you won’t cross. For example, would you punch an athlete in the face if they asked you to? Give them a 90-minute full body massage in your underwear because it “helps my shoulder”? My goal in writing this post is to help you define that line so you can stay true to it.
Now, let’s go for a walk
“I DON’T GIVE A SHIT WHAT ‘THE EVIDENCE’ SAYS! HE WANTS ACUPUNCTURE, YOU FIND HIM SOME DAMN ACUPUNCTURE! OR ELSE YOU CAN FIND YOURSELF A NEW JOB SOMEWHERE ELSE!”
As I said, I work in this setting. I get it. These kinds of exchanges happen. One might say this person SHOULD find a new job. I will say that you don’t understand how hard that is, especially if your former employer is now bad-mouthing you to anyone who will listen. If the athlete really wants acupuncture after I have gone through my lecture on its limitations, I will have to find them a provider. But I will NOT perform it myself.
Let’s look at another scenario. It is minutes before their event and the athlete is in a tailspin. They are panicking about their shoulder. “It’s not RIGHT. I’m going to FAIL! What do I DO?!” The famous “Pirin” scene from the wonderful 1995 remake of The Birdcage gives a great example:
In the scene, Albert is in a panic before a show. He demands some Pirin to calm him down. Turns out that Pirin is “just aspirin with the A and the S scraped off”. Whatever it takes to get them out there focused on the sport. Again, I get it.
And sometimes there is just the ritual. Often times an athlete will use something “questionable” more as simply part of their pre-competition routine. Again…
I get it
But there is a catch…
To the surprise of many, I will not categorically reject ALL placebo use for elite athletes as “wrong”. But there are things you really need to consider. The ways these things infiltrate a training room are nefarious and need to be addressed proactively and head on. But before we can do that, we need to identify exactly what the problem is. We need to realize that we don’t actually do “whatever the athlete wants”. I have said before many times, you need to consider exactly what you are doing and ALL the implications.
Settle the score
In order to do all of that, I have created a scoring system for the use of placebo-based treatments in elite athletes.
Please note, this is in the context of “A desperation attempt to get an athlete back out there”, NOT for its daily use in non-elite athlete applications.
Use the questions below to create a “score” for the intervention that you are considering using. The higher the score, the more questionable the application. What you will notice pretty quickly is that every intervention will have its own minimum score (some higher than others) but how the intervention is applied can make that score much worse.
Think I’m being lenient about placebos? Go ahead. Run a treatment through the system. See how hard it is to get an “acceptable” score of 13…
Here is the scoring system:
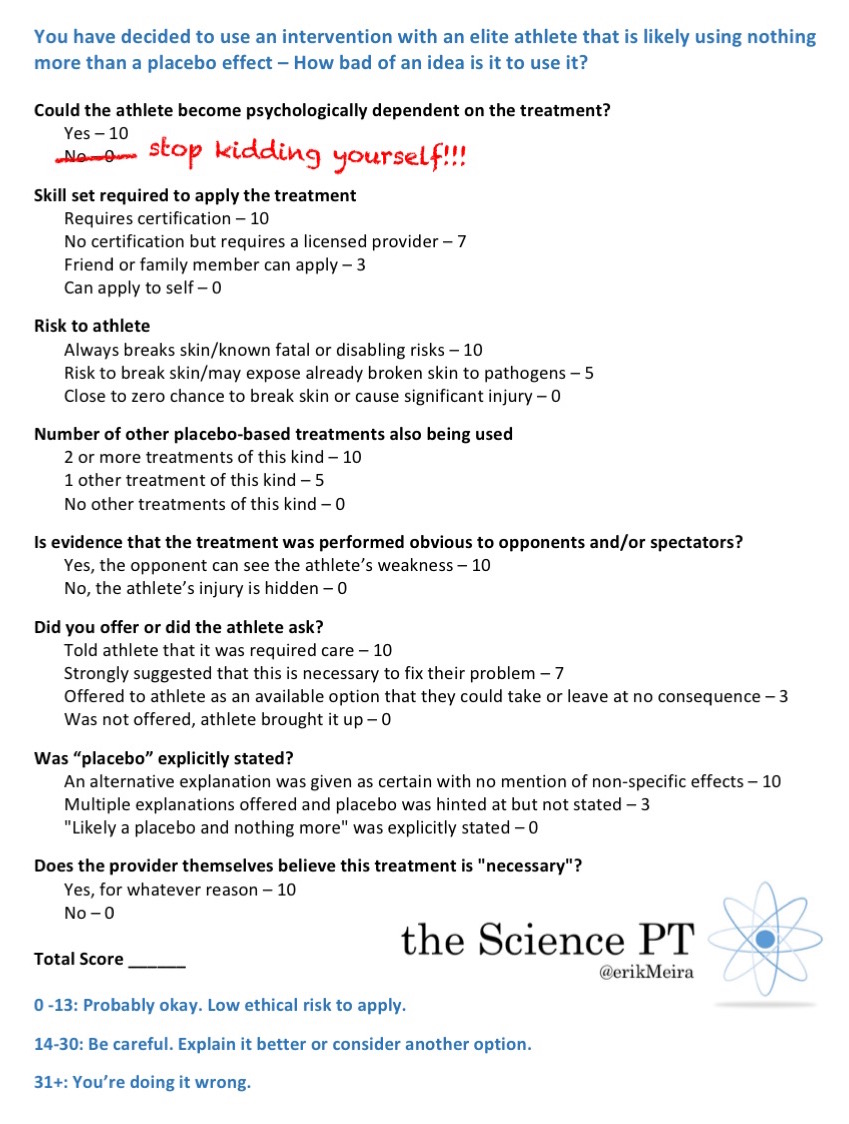
My Placebo Scoring Sheet. Click to embigganate…
Breaking down the scoring system
There is a lot to consider in that scoring system. Most of it should make sense but let’s explore each heading.
Could the athlete become psychologically dependent on the intervention?
There is only one answer to this: Yes. And it gives you a whopping 10 points right off the bat. The first thing that you must accept is that there is a strong potential for psychological dependency. You must ask yourself, “Would I prefer their potential dependence on THIS, or would it be better for them to become dependent on something else?”
Look, they’re going to depend on something. I’m not judging that – they ALL get a 10 for the dependency. But you need to be thinking about it as you move forward.
Skillset required to apply the intervention
First, this comes to a resource issue. How much do you have to pay for training? Not to mention other potential costs like tool rentals and disposal fees. Assuming you have unlimited resources as many athletic programs do, this may not be much of an issue.
But what about your time which is also a limited resource? I’m often asked how I know so much about hip pain or ACL rehab. Well, for starters, I didn’t waste a bunch of my time and brain capacity sitting in a dry needling course. So there’s that.
But this also is where the dependence can expand into more of an issue. Does the athlete need to find the ONE certified person who can do this intervention? Can any professional do it? What if a teammate is all that is needed and it can be applied anywhere, not just the training room? Of course, if the athlete can do it to themselves whenever they want, that is at least not dependent on another person.
Risk to the athlete
Now many of you will say that in modern practice, even skin breaking procedures are of minimal risk due to standards of practice. Sure, but there is a risk and that risk is often infection which can be a big deal. So if the benefit is likely based in placebo, which can be applied to other treatments, why add that risk?
Also remember that athletes present with broken skin all the time from simple lacerations and abrasions just from playing their sport. How safe is it to dunk them in that full body immersion tank? Is that tank REALLY clean? It’s not like MRSA has ever run through an athletic team before…
Number of other interventions of this type also being utilized
Ok. You did one of these interventions to the athlete. Are they also getting cupping, and kinesiotherapy tape, and dry needling, and massage, and so on? That is a lot of mental crutches for one athlete to require. I would be very concerned with how coddled your athletes may have become.
I have a rule for injured athletes:
You are going to work much harder when you are injured than when you are healthy.
If you come to me, I’m putting you to work. I don’t care if you are immobilized. Foot fracture? Hit the upper body workout. Work the other leg as well. No lying around getting a massage. You know what works well for most athletic injuries?
Progressive, systematic load management
And that takes work. And yes, the athlete will feel some pain. Learning to suck it up and deal with some pain is not a bad skill for an athlete to develop. As Patrick Swayze said in Roadhouse, “Pain don’t hurt.”
Is evidence that treatment was performed visible to opponents and spectators?
It absolutely blows my mind that less people consider this:
The last thing you want to show your opponent is where you are injured!

I mentioned this to a lacrosse player. She smirked, “Yeah, if I see that colorful tape on an opponent’s knee, I’m gonna hit them there.” Showing your vulnerabilities to an opponent is one of the dumbest things you can do. Hide it don’t flaunt it!
Also consider the spectators. Are you now spreading this questionable treatment through the general population like a virus, wasting resources such as time and money not to mention dependency? And if for no other reason, think twice before doing it just so you don’t get publicly called out and embarrassed by the scientific community for promoting (intentionally or not) a questionable practice.
Now sometimes something like tape will be used more for decoration, or a representation of the athlete’s “armor”. The athlete says, “I just think it looks cool.” That’s different. Athletes are weird sometimes with their music and their fashion and their being 19 years old and stuff.
Did you offer or did they ask?
Here’s where I get a little irritated. “My trainer said that I NEEDED to have cupping for my shoulder pain. If I don’t report to the training room for it, I am seen as ‘non-compliant’.” I have also heard of coaches requiring all their athletes to participate in full body ice baths after every practice or to put kinseotherapy tape on anyone who has pain. I’m sorry, not only is that completely unethical, that is actually ILLEGAL. You cannot force someone to receive a “treatment”.
And then there is the next worse thing: Making the athlete think that this treatment is required in order to recover. You are literally building dependence with this line of education. And, you’re wrong. But we’ll get to that in a minute.
Contrast that with saying, “I can do this if you want.” At least you aren’t pushing it on the athlete. An example of this is saying, “Do you want to throw an ice pack on your knee?” even though this is not an acute injury. No, this by itself does not make providing the treatment “OK”; you need to look at the rest of the score.
If the athlete brings it up, well there is nothing you can do about that. Unless…
Did they come to your program already getting these things? Or was this baggage that YOU added to the athlete’s care?
In my experience, the way an athlete gets one of these treatments for the first time was that someone at some point said to the athlete, “What’s the harm?” and then threw everything they had at them. Try not to add these types of things in the name of “might help”. If some other provider has added them, work hard to take them away.
Was “placebo” explicitly stated?
The first situation, where you actually make a completely different claim as to what the treatment does (most times in the name of “increasing blood flow”), is just misleading. Don’t do that. Maybe you actually believe this explanation – again, we’ll get to that. But what if you actually accept that the treatment may be nothing more than a placebo?
Did you say actually SAY placebo? “Well I told them that there were a couple different possible explanations and the effects could be psychological.” Ok, that’s better, but what did the athlete hear? “Psychological”. What does that mean to them?
The word to use is “placebo”. Explicitly say it. They know what that means. All you have to do is tag it on the end. I have seen that word added as an afterthought after the athlete had agreed to the intervention and their change in disposition is abrupt:
“Wait. Placebo? Yeah, never mind. I’ll pass.”
In my experience, athletes actually don’t like to use something once they hear that word.
AND DON’T ARGUE THAT THE TREATMENT DOESN’T DO ANYTHING!!! That’s not saying the same thing. They know it does SOMETHING. They felt it.
It DOES do something and there is a word for that thing: Placebo
Does the provider themselves believe that the treatment is necessary and more than placebo?
So this is a deeper problem. Scoring a 10 here means you probably scored a 10 several other places on this sheet as well. Why do you believe this? It can’t be, “Because I see people feel better afterwards.” That is an unacceptable reason to do something because LOTS of things fall under that category. But let’s say that you believe the explanation that you have heard elsewhere about bloodflow or trigger points or whatever. Fine. I’m not even going to comment on that because whether or not that is true is actually irrelevant.
The point is that you should stop and think about OTHER explanations regarding what may be going on. Most of these treatments don’t have any proof that what they claim to do is actually happening. Why aren’t you at least skeptical? Hell, there are legitimate alternative hypotheses to how gravity actually works!!!
What exactly is your problem? Why are you so damn certain about something with so little evidence? Shame on you. You science bad.
What is your gameday “trinket”?
Let’s go back to “Pirin” – the spiraling athlete who is panicking right before competition starts. This is not the athlete’s fault. This is YOUR fault. YOU failed to prepare them for this. Now your only option is the “Pirin”. This has nothing to do with gameday. This has to do with the day you first met that athlete.
Every injured athlete I work with gets the same conversation with me early in their rehab. I would have the same conversation with EVERY athlete, injured or not, when I had my first meeting with them if I was on full time staff with a team. This is the conversation I have:
I talk about how sport has a lot of psychological components to it (they know this). I also talk about how on gameday emotions and anxieties run high (they also know this). We discuss how this can amplify their thoughts regarding a recent injury or a previously achy spot. But that injury didn’t change right then and there; that achy spot didn’t change. THAT isn’t the problem. The actual problem is a loss of control of their anxiety and their emotions.
So then I ask them, “What is your ‘trinket’?” Like a charm or what the Louisiana Creoles call “gris-gris”. What is the metaphorical thing that the athlete will rub to bring their emotions into check? Like a security blanket, a meditative focal point, a thing to psychologically and emotionally center them. It is almost like “going to a happy place.”
If they don’t have something, I offer suggestions. Listening to a particular song they really like (What I would listen to before matches in high school – WARNING: Do not click link if you have a heart condition). Sitting in a quiet space. Doing a series of movements (I had one guy who did pushups before every match). Engaging in a series of isometric contractions (shown to reduce pain systemically). Drink a glass of water. Use a physical item like a temporary tattoo they put on as their “armor” or a rubber bracelet that reminds them to “chill”. Even something as “silly” as a lucky coin or turning their socks inside out.
There are literally thousands of possibilities that would all score very low on my scoring sheet. It is a VERY long list of options before you get to anything like cupping. Get creative. Quit being lazy. If they need a psychological crutch, overtly and explicitly give them a psychological crutch. Be intentional.
My final point here is that these options are discussed long before that day with a rational, informed athlete and then continuously reinforced throughout their care. THIS is being patient centered instead of being patient placating. This also prevents the tirade from an administrator to “FIND HIM SOME DAMN ACUPUNCTURE!”
And stop believing your athletes are stupid scared children who need to be coddled and told fairytales about how things work just to placate them. In other words, stop being a patronizing, paternalistic douchebag. The fact that they are ignorant does not mean that they are stupid.
In summary…
- Dammit that was a way longer post than I wanted to write – I hate you people
- Working in elite sports is a complex mess of very real injuries and very real psychology
- You actually don’t do “whatever the athlete wants”
- There are many consequences to what we offer an athlete at many different levels
- Manage the athlete’s expectations throughout the year in a patient centered and ethical way
- Stop being a patronizing, paternalistic douchebag
The featured image on this post is “PlaceboScoring” by Erik Meira and is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License

Also included on this post is “InjuredWorkHard” by Erik Meira and is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License adapted from “getting-huge” by Eric McGregor.
{kind=link}
Also included on this post is “InjuryReveal” by Erik Meira and is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License adapted from “KinesioTaping” from Wikicommons.
{kind=link}
{kind=link}